
Breast Augmentation Incision Types

Breast implants are usually inserted through an incision under the breast or around the nipple
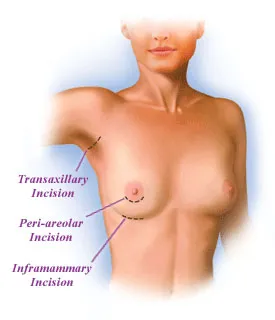
The two most common incision locations used in breast augmentation surgery are in the crease where the breast meets the chest (inframmamary fold incision) and around the nipple (peri-areolar incision). The incision is made less frequently in the armpit (transaxillary incision) or around the belly button (transumbilical incision).
Incisions for Saline and Silicone Breast Implants
During breast augmentation surgery, your plastic surgeon will make the incisions through which to insert the breast implants and expand your chest contours. Incisions for saline breast implants are usually only about an inch long, while the incisions for silicone gel breast implants are generally a little longer. This is because saline implants are rolled up, inserted empty and filled with sterile saline solution using a syringe, allowing your surgeon to use as small an incision as possible. On the other hand, silicone implants are pre-filled with the silicone gel.
With both types of breast implants, scars left as part of the body's natural healing process are usually small and well-hidden.
Your surgeon will discuss his or her recommendation for an incision type during your consultation prior to surgery.
Inframammary Fold Incision (crease beneath breast)
Crease Incision
- Currently the most common implant placement.
- Surgeon works close to the placement site.
- Scar is very discreet.
The inframammary fold incision, or crease incision, is probably the most common incision type currently used for breast augmentation. The incision is made just above the crease where the breast meets the chest. The implant is then inserted upward through the incision to the placement site. Saline implants are filled with sterile saline solution after being placed. The scar should be very discreet and not visible unless the breast is lifted upward.
The crease incision can be used for subglandular, subpectoral or submuscular placement of the implant. Using this incision, your plastic surgeon can work in close proximity to the placement site and place the implant precisely. The implant can also be removed through a crease incision if necessary due to a complication. Virtually all revisions, such as to correct capsular contracture, can be made using the crease incision.
The surgeon may have to create a new crease when there is a large increase (or decrease) in size, or when the patient lacks a natural crease. When large implants are used, the crease is usually lowered in order to center the breast implant behind the nipple. Your plastic surgeon will use his or her skill and experience to estimate the position of the new crease and make the incision so that the scar will be hidden in the new crease. Rarely, the incision may be misplaced, possibly causing the scar to be visible on the breast or on the chest below the breast.
Peri-areolar Incision (nipple)
Nipple Incision
- Commonly used for breast augmentation.
- Surgeon works close to the placement site.
- Scar blends in at the edge of the areola.
The peri-areolar incision, or nipple incision, is one of the most common incision types used in breast augmentation surgery. The incision is made at the perimeter of the areola, which is the darker skin surrounding the nipple. The implant is then inserted through the incision to the placement site. Saline implants are then filled with sterile saline solution. The scar blends in with the change in skin tone from the areola to the lighter skin of the breast.
The nipple incision can be used for subglandular, subpectoral or submuscular placement of the implant. Like the crease incision, the nipple incision allows the surgeon to work close to the placement site and precisely place the implant. If necessary due to a complication, the nipple incision can be used for revisional procedures or implant removal.
The nipple incision requires the use of a protective sleeve to prevent contamination of saline implants from bacteria in the lactiferous sinuses, which are located behind the nipple. Prior to being inserted, the breast implant is rolled up and placed into the sleeve. The sleeve is removed after the implant is placed into position.
Your surgeon will almost certainly recommend the nipple incision if you are having a breast lift, or mastopexy.
Transaxillary Incision (armpit)
Armpit Incision
- Less commonly used than the crease and nipple incisions.
- Surgeon has to work further from the breast.
- No scarring on or around the breast.
The transaxillary incision, or armpit incision, is less frequently used than the crease and nipple incisions. The incision is made in the armpit and a channel is created to the breast. The breast implant is then inserted into the channel and put into place. The scar is small and well-hidden in the skin of the armpit.
The armpit incision can be used for subglandular, subpectoral or submuscular placement of the implant. This incision is sometimes preferred by patients who desire no scarring on or around the breasts. However, the armpit incision is more difficult for surgeons because they have to work further from the breast than with the crease or nipple incisions. Some surgeons use an endoscope (a tube fitted with a surgical camera) in placing the implant using this technique.
Transaxillary incisions usually cannot be reused in the event of a complication. If a complication occurs that requires revision or removal of the implant, your surgeon will probably use a crease or nipple incision.
Transumbilical Incision (bellybutton)
Transumbilical Incision
- Less common than the other incision types.
- Surgeon works very far from the placement site.
- Scar is practically undetectable.
The transumbilical breast augmentation (TUBA) incision, or bellybutton incision, is the least common of the incision types covered in this section. Few surgeons currently perform this incision, and it can be difficult to find a surgeon who is experienced with the technique. The distance from the incision site to the breast can make it difficult for the surgeon to get the implant properly into place. This incision is not used for silicone gel implants.
The TUBA incision is made at the rim of the bellybutton. Using an endoscope (a tube fitted with a surgical camera), the surgeon creates a channel through the subcutaneous fat beneath the skin to the tissue behind the breast. The breast implant is rolled up, inserted through the channel to the placement site and filled with saline. Once the implant is in place and filled, the surgeon uses the endoscope to examine the implant prior to closing the incision.
The TUBA incision can be used only for subpectoral or submuscular placement of the implant. Like the armpit incision, the TUBA incision usually cannot be reused in the event of a complication that requires revision or removal of the implant. If a complication occurs, your surgeon will probably use a crease or nipple incision. Rarely, this technique can leave "V tracks" on the stomach.
Despite the distance between the incision site and the breasts, breast augmentation performed using the TUBA incision is actually considered to be less invasive than the other incision types. The scar is practically undetectable because the skin of the abdomen has a higher degree of elasticity than the skin around the breasts or in the armpit. This technique also usually results in less discomfort following surgery and a shorter recovery period.